At about 5pm on Thursday, I shut down my laptop on the day’s work for the very last time, or so I imagine. We never really know what the future has in mind. I’m calling it early retirement, although I’m a few years away from getting any form of pension.
Sitting in an armchair drinking coffee at 11:30 on a Wednesday morning is a strange experience. The prospect of being able to do this would have seemed like nirvana this time last year. Although not quite nirvana now, it does feel pretty good.
I’ve only been ‘retired’ for four days, and I know that this carefree high isn’t going to last forever; however, I’m enjoying it while it lasts! I have been working, without a break, for the last 46 years and as time passed, living to someone else’s timetable became increasingly constraining. The freedom to work, or not, when you want, to take a holiday when you need, is so liberating. I don’t underestimate the privilege of having this opportunity; I’m aware that so many of us don’t have the choice to stop working, and I’m incredibly grateful.
So, What Do I Do Now?
I could fill a small book with all the ideas I’ve had, things I’ve wanted to make, and projects that I haven’t started, never mind finished. My first priority is to get well, or at least to manage my antidepressant withdrawal as best as possible. Not spending over eight hours a day sitting behind a desk will help. Other than that, I’m going to start some much-needed work in the garden by planting some vegetable seeds. Gardening should help my physical health and, if all goes well, our diet.
I’m desperate to get back on my bike. I don’t like using the car for local journeys. Whereas I used to enjoy cycling to the supermarket and loading up my panniers, driving to the store feels like a chore. I’ve written about my box camera project, which I seem to have been planning for years! I’m eager to start, but I keep reminding myself to take it slowly.
The Elephant Is Still in the Room
My withdrawal symptoms have fallen into a very distinct pattern. For two or three days, I feel okay; my hands and legs are uncomfortable, but with the aid of paracetamol, I get a reasonable night’s sleep.
This is generally followed by about a week where the effects slowly peak and then tail off. I get the same several waves of pain each day, most noticeably overnight and in the morning. Sleep goes from difficult to nonexistent, and I find myself talking to the pain, as though telling it to f*** off might make a difference. Of course, knowing I don’t need to get up for work the following morning makes a big difference.
As of this moment, on this Wednesday morning, it’s not bad. I’ve all but drunk my coffee, and I need to go to the store, although for now my bike stays in the shed.
Take care. N.
For Professional Advice
Dr Mark Horowitz’s website offers the most practical, professional advice I’ve found online. The academic papers are impenetrable to the nonprofessional. But he has useful links to newspaper articles which explain things in layman’s terms. The UK mental health charity, Mind, is also a good resource.
I’m not a medical professional. The following is my personal experience. Please talk to your Doctor before you change your medication or take painkillers.
If you’ve ever avoided writing a letter, you realise that the longer you wait, the harder it gets. It sounds as though I’m making excuses; it wasn’t that I didn’t want to write, if I’m honest, I haven’t known what to write. It may not have come across, but when I’m writing about my antidepressant withdrawal, I’ve tried to maintain a note of optimism and, in my own clumsy way, inject a little humour. However, as last year came to an end, I couldn’t summon either. My 62nd year has been one of the worst, and it seems as though there’s nothing I can do about it.
When I took my last tiny dose of Amitriptyline on the 20th July 2025, I knew that there were going to be withdrawal effects, that at times they might be unpleasant, and they were likely to hang around a while. I wasn’t wrong. What I hadn’t expected was that almost six seven months later, they would be having such a significant impact on my life and that they would, if anything, be getting worse.
So, I put off writing, telling myself that I’d pick it up at the end of January; today is the 14th February, so judge for yourselves how well that went.
I’d like to think that I’ve now come to terms with that new reality, but being honest, I haven’t really. Back in July, I remember reading that the 5% of antidepressant users have withdrawal symptoms that last longer than nine months. But there are dozens of antidepressants and millions of users; we’re all different. I rationalised that although most of the remaining 95% would have been taking the drugs for less than my 25 years, some had to have been. Maybe Amitriptyline wasn’t one of the worst drugs, and I couldn’t be that unlucky, could I?
In the cold light of January, I read the summary of a paper detailing the reality of how many sufferers experience side effects for multiple years; that many are far worse than I have experienced (so far). Missing both the Amitriptyline and the sunlight, my mind started to wonder whether not only could this last more than my mythical nine months, but it could get significantly worse.
The Symptoms
In the abstract, it’s interesting how the symptoms have changed. The first few weeks of withdrawal were dominated by headaches. Amitriptyline takes about seven days to leave the system. So in those first few days, the headaches were the actual withdrawal of a drug my brain had become used to over the previous 25 years. They were followed by a range of symptoms (I wrote about them in MHH #4) affecting every part of my body, from balance and tinnitus to itchy skin and insomnia. There’s a very comprehensive list on the Mind website; I’ve ticked off most of them.
The constant, since I started cutting down the Amitriptyline over a year ago, is the numb pain in my extremities, mainly my legs. At first, it was similar to pins and needles, annoying but easy enough to ignore. It transitioned through restless legs and has now developed to become a dull, constant pain that affects my whole body from my toes to a patch on the top of my head. It never recedes completely. At times, if I’m distracted, it’s easy to ignore, and then there are the other times, when it is everything. Nothing can quieten its presence.
There are the large waves and the smaller waves within them. The best way I can explain it is like an electric current running through my body. The large waves last a few days; the smaller waves, a couple of hours.
The Solution
This is probably a good time to remind you that I’m not a Doctor. These are my conclusions from my personal experience. Discuss your symptoms with your doctor.
It should have been obvious sooner that any substance that affects our perception is, to a larger or smaller degree, changing the chemistry of our brain. That could be coffee, antidepressants, or painkillers. This is the same chemistry that our body is trying to rebalance. It doesn’t seem a stretch to think that this could slow that rebalancing. If you have a medical diagnosed imbalance, that’s one thing, but if we’re self-medicating even to ease symptoms, are we hindering that rebalancing? Of course, the effect could be negligible, or a price worth paying. I’d love to have the medical knowledge to research it.
So, the options are limited. I find the headaches the hardest to cope with. On average, I get two bad headaches a week. As I understand it, Paracetamol is one of the safest commonly available over-the-counter painkillers. Unfortunately, it doesn’t have much impact on my headaches, so for those, I take Ibuprofen, which does help, but taken long-term can damage the kidneys, so I don’t like taking it frequently.
The pain is generally worse in the mornings and evenings, so I take two 500mg paracetamol tablets before I go to bed. Generally, they help me to get to sleep. Then I take two more if the pain is bad when I wake up in the night (as long as four hours have passed). I don’t take painkillers during the day, unless in the most exceptional circumstances.
I mentioned in MHH #5 that I’d taken Co-codamol (which contains codeine and can be addictive). My pharmacist had said it was okay to take one tablet each night. That didn’t chime with what was clearly written on the box. When I next saw a GP, I mentioned it, she was emphatic that it is far from okay and went so far as to insist that I don’t take it.
The Effects
Antidepressant withdrawal syndrome has had a huge impact on my life. If I weren’t able to work from home, I would have had to stop working some months ago. As it is, there are many days I have been less productive than I need, but I’m fortunate that I can catch up when I feel better. However, I have decided to retire early. I have a demanding job, and I know that I’m not turning in my best work; there’s only so long you can make excuses. I’m not old enough to get a state pension, but my wife is working, and I’m not a huge spender, so as long as I’m careful, my savings should last.
I didn’t have a busy social life, which was not great, but okay, but now it’s virtually nonexistent, which isn’t okay. A couple of lovely close friends have kept in touch, and I’ve promised myself I will treat them both when I can. Apart from that, life is quiet.
I have so many plans. There is so much I want to do. When I hit 60, I realised that there is far more I want to do than I have time for; so these days spent sitting on the sofa looking out of the window are not easy.
If you’re entering withdrawal and looking for reassurance, then I feel I should apologise. Today, you’ve come to the wrong place. I don’t have a life-threatening illness, and yet this withdrawal has all but stolen my life. It’s difficult not to feel just a little cheated.
Dr Mark Horowitz’s website offers the most practical, professional advice I’ve found online. The academic papers are impenetrable to the non-professional. But he has useful links to newspaper articles which explain things in layman’s terms. The UK mental health charity, Mind, is also a good resource.
I’m not a medical professional. The following is my personal experience. Please talk to your Doctor before you change your medication or take painkillers.
In what could be an outtake from a bad episode of Star Trek, I’m talking to my Mac, trying to find the form of words that will persuade it to add punctuation to my latest blog post. I have tried the dictation in the past, but whatever magic Apple has worked in the interim, it’s far more accurate.
I established that I need to say ‘period’ instead of ‘full stop’, and I can cope with that. However, if my USA friends have a secret word for ‘paragraph’, I haven’t found it. (update: apparently, the key is to say ‘new’ paragraph)
The ongoing side effects of antidepressant withdrawal forced me to look for alternative ways to amuse myself. A new discovery is how much I enjoy writing, particularly in this blog. I continue to be dreadful at it; that’s a given. I rewrite each one several times. But my lifelong tussle with the written word is something I came to terms with a long time ago.
Almost no one, other than a few lovely friends, reads it, but that doesn’t diminish the pleasure of the writing. Photography is too personal; if the results of a shoot are disappointing, I can’t shake it off. I have carried them with me for years. I appreciate that it shouldn’t be like that, but that’s how it is. Writing is akin to a hobby. One that I don’t mind not being good at. I enjoy the process, maybe I’ll do better tomorrow, maybe I won’t, and that’s OK.
I’m far too easily distracted to concentrate for any length of time on a laptop. So, inspired by the author Mark Boyle(The Way Home), I picked up a pencil and a pad; the simplicity of it is refreshing. No logging in, no apps, no syncing, no staring at another screen, and no distractions. With pencil and paper, I can write anywhere.
I’ve gotten slightly off track. I’ll talk about the joy of writing some other time. So why dictation? Well, I have developed a pain in my right hand. The difficulty when going through something like antidepressant withdrawal is that its all-encompassing nature results in your blaming it for every ache and pain. However, in this instance, I am beginning to think this is more likely a simple case of RSI (repetitive strain injury). Good in a way, but the only treatment for RSI is rest. Writing has become a sanctuary, and this seems an unnecessarily cruel blow.
The world is still out there. It is waiting. We will return to it. Remember that!
I have tried writing with my left hand, which was a short-lived experiment. So, here I am in a room alone, talking to my laptop. Speaking my thoughts out loud before they are fully formed isn’t comfortable, and I already doubt that dictation is going to last. But the inability to write is one of the most frustrating aspects of my current ill health, and I’d love to find a solution.
The challenge, as always, is to stay positive. It is now over four months since I stopped taking Amitriptyline; over a year since I started tapering. The discomfort and the poor sleep. The repetitive daily routine of work, cook, TV, and bed seems as though it may last forever. Every so often, I have to stop and remind myself that this will come to an end. That this is temporary. You will spend time with friends; you will be able to walk with carefree abandon; you will ride the bike that taunts you whenever you go to the shed. The world is still out there. It is waiting. We will return to it. Remember that!
For Professional Advice
Dr Mark Horowitz’s website offers the most practical, professional advice I’ve found online. The academic papers are impenetrable to the non-professional. But he has useful links to newspaper articles which explain things in layman’s terms. The UK mental health charity, Mind, is also a good resource.
I’m not a medical professional. The following is my personal experience. Please talk to your Doctor before you change your medication or take painkillers.
It’s Sunday morning. I can’t see the clock, but I can tell it’s late.* I try not to move a muscle. It’s the sort of game you play when you’re six, not sixty. I took some ibuprofen at about 7:30 this morning, and it’s beginning to wear off. I can feel the numbness coming on, but nothing really hurts yet. My six-year-old logic is that if I lie perfectly still, then maybe I won’t feel the pain. Not so long ago, I would have been appalled to be in bed at this time, but a lot has changed since then.
I write and rewrite this blog in my head. Writing doesn’t come naturally to me, so on the rare occasions it flows, I need to get it on paper before it disappears. It’s already slipping away. How did this paragraph start? I need a pencil and some paper, but I don’t want to move.
“I’m not fighting anything… I’m not part of the resistance, more a disgruntled conscientious objector”.
I’m going to have to move soon. At one time, weekends were for fitting in the things I wanted to do, free from the commitments of someone else’s timetable. I couldn’t lie in bed; I had stuff to do. Now life is far simpler; weekday or weekend, it’s much the same. Get through the day as painlessly as possible, still be here tomorrow, that’s my job for today. Some people describe fighting pain. I’m not fighting anything; it’s happening, and I’m putting up with it. I’m less part of the resistance; more of a disgruntled conscientious objector.
Sticking with this tired metaphor, it’s been nearly four months since Amitriptyline ceded control of my brain to Fluoxetine and my neurons, the citizens of my grey matter, are far from happy. I started counting in days and then weeks, the way you do with a baby. ‘Ah, how cute. How old? Four months, lovely!’ Or not so lovely in this case. I can’t consider the idea that this battle may still be waging after a year.
Too Many Painkillers!
The painkiller is wearing off. My head hurts. I’ve made a commitment to myself not to take painkillers during the day. I have a fear of taking too many, and I need them to help me sleep.
If I need to, as I did last night, I take ibuprofen before I go to bed. That allows me to sleep sometime between midnight and 3 am. When I wake, I usually spend the first few minutes, as I am now, trying to pretend it’s not happening; it always is.
When I need to, I take two Co-Codamol, but be careful, they’re not for everyday use. However, last night was one of those times. I go to the bathroom, stare out of the window for a while, and have a stretch. I discovered that the muscle numbness and pain I’ve been trying to describe for the past few months is called akathisia. It’s the devil and my constant companion.
The Co-Codamol takes about 45 minutes to start having an effect. I’d like to read, but I can’t concentrate. I’ve tried listening to a podcast, but using earbuds with a headache makes it feel as though the sound is being injected into my brain. At some point, I nod off.
I woke about 6.30 am and dozed for a while. Took another ibuprofen, had breakfast, made my wife a cup of tea, and read the news. They’re reporting that ‘a number’ of people have been stabbed on a train in Cambridgeshire. And apparently, JD Vance believes his Muslim wife should convert to Christianity. Welcome to the world in 2025.
I go back to bed and sleep for a while. So here I am, having less success at pretending it’s not happening.
Take care out there.
Co-Codamol can be addictive and could cause withdrawal symptoms. I’m very uncomfortable taking them and do so only, maybe, once a week. Please don’t do what I do; talk to your Doctor.
Dr Mark Horowitz’s website offers the most practical, professional advice I’ve found online. The academic papers are impenetrable to the non-professional. But he has useful links to newspaper articles which explain things in layman’s terms. The UK mental health charity, Mind, is also a good resource.
I’m not a Doctor. The following is my personal experience. Please talk to your Doctor before you change your medication.
This is the fourth post in a series detailing my experience of antidepressant withdrawal syndrome, concentrating on the side effects. Starting in November 2024, I tapered down my use of Amitriptyline over eight months. At the same time, starting to take Fluoxetine (Prozac), originally 40 mg/day, I now take 30 mg.
I finally stopped taking the Amitriptyline three months ago, with my final dose of 2 mg. My symptoms haven’t changed significantly since MHH-3 last month, except for the bouts of pain/ache/restlessness (see below), which are far worse.
In each post, I’ve referred to the side effects, but I haven’t really gone into any detail about how they affect me or how they’ve changed over time. Everything I’ve read indicates that we all experience side effects in different ways and to varying degrees.
“My head hurt so profoundly that it made me incapable of doing anything other than sitting still, in a quiet room with my eyes closed”.
The severity also seems very dependent on several factors, including:
How long had you been taking the medication before you started tapering. I took Amitriptyline for 25 years. The dose varied; at one point, it was 50 mg/day.
The dose when you started tapering. I started tapering from a dose of 25 mg/day.
How quickly you tapered. Both the size of the reduction and the time between steps. What is known as hyperbolic tapering (very slowly) seems to be the current accepted best practice. I might post about that in the future. This guide from the Royal College of Psychiatrists is helpful.
The time you’re taking the medication seems less significant the longer you’re on it. In other words, stopping after four months should be easier than after twelve months. The difference between, say, ten years and twenty years may not be so great.
Please remember, this is my layperson’s understanding of complicated medical data. Always discuss your medication with your Doctor.
How Withdrawal Affects Me
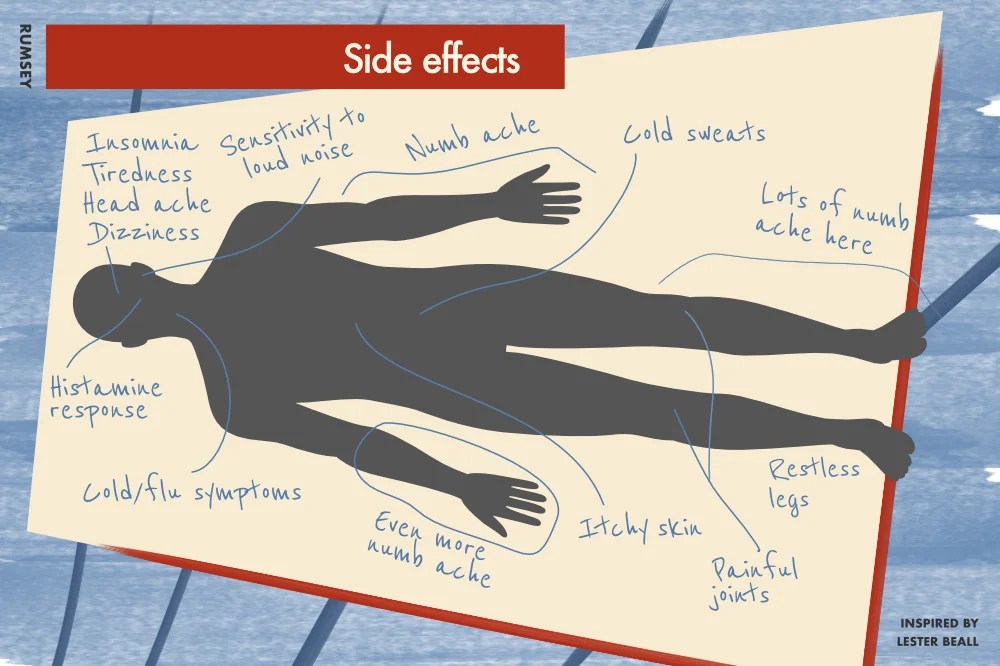
The UK mental health charity, Mind, produces a list of common withdrawal side effects which correlate closely with my personal experience. Headaches, for example, were very significant in the early stages but have become far less pronounced over time.
Joint pain, aches, numbness and restless legs: I’ve always struggled to describe this feeling. It’s very similar to the drained ache you get with flu, at times it feels as like an electric shock (update: since posting, I discovered this condition is known as akathisia). My lower legs and forearms are most affected, but recently it’s more of a whole body thing. For me, it’s by far the worst side effect.
Insomnia: Some of my inability to sleep is a result of the aches and pains, most noticeably in my legs. But there also seems to be an element of standard insomnia thrown in for good measure.
Tiredness: This is obvious, I suppose. But the overwhelming fatigue has the largest impact on my day-to-day activity levels.
Cold/flu symptoms: Cough, sore throat, and a blocked nose.
Itchy skin: I seem to have developed a more pronounced histamine response. I normally suffer from mild hay fever, but that was far worse this year. I get very itchy skin, although a daily antihistamine tablet mainly keeps it at bay.
Dizziness: Thankfully, this has largely disappeared in the last couple of months.
Nausea: Not too bad. It comes in waves, but subsides very quickly.
Headaches: Withdrawal was heralded by the most overwhelming headaches, hence the name of this series. My head hurt so profoundly that it made me incapable of doing anything other than sitting still, in a quiet room with my eyes closed. Thankfully, they’re far less frequent and much less severe.
Sensitivity to certain noises: This is a weird one. I’ve become very sensitive to certain noises. Imagine clanging a saucepan lid on something hard, that’s the one!
In writing this list and trying to describe each of the symptoms, I realise that in the main they’re all connected to the nervous system, but I guess that makes perfect sense. Antidepressants change brain chemistry; my brain is now trying to readjust, after 25 years, to the absence of Amitriptyline.
As I’ve mentioned before, my nagging concern is that maybe the side effects of withdrawal stopped some time ago, and what I’m experiencing is a reaction to the Fluoxetine. I don’t think that’s the case, but it would be good to know for sure.
Unfortunately, I started taking Fluoxetine at the same time I cut down the Amitriptyline. Changing two independent variables concurrently is never a good idea. Then I’m not a psychological experiment, or am I?
Dr Mark Horowitz’s website offers the most practical, professional advice I’ve found online. The academic papers are impenetrable to the non-professional. But he has useful links to newspaper articles which explain things in layman’s terms. The UK mental health charity, Mind, is also a good resource.
It’s important to say, I’m not a Doctor. The following is my personal experience. Please speak to your GP before you make any changes to your medication.
Have you thought about why some people, often young women, are driven to cut themselves? Taking a blade and deliberately cutting into your own flesh seems so counter to everything we think of as normal, certainly in the Western culture I grew up in. I find it difficult to comprehend.
“I’m moving spread-eagled towards a wall, a very hard, rough concrete wall.”
But at three in the morning, when my body really aches, when I get that indescribable feeling between a numb ache, a pain, and an electric current running through everything, I always imagine the same scene. I’m running, but not running, that wouldn’t make sense. I’m moving spread-eagled towards a wall, a very hard, rough concrete wall. Every part of me hits the wall at the same time, and the feeling stops, just for a moment. It’s quiet, no, it’s silent, everything is silent, and I relax. That feeling doesn’t last long, almost no time at all. That’s what I imagine cutting is like: a release. A way to stop everything, without stopping EVERYTHING.
Don’t worry, I’m not in danger of cutting myself or running into a concrete wall; apart from anything, I’m far too squeamish. I’m pleased to say, I have no wish to hurt myself in any way. But, strangely, the thought is always the same: perhaps it’s my subconscious telling me something.
A Quick Recap
At the end of the last post, I was four weeks into my life, after 25 years, without Amitriptyline. A month later, and disappointingly, very little has changed. I’m still taking 30 mg of Fluoxetine daily, and I’m still experiencing the same side effects.
Bizarrely, the worst aspect is not the side effects themselves, but how they affect my sleep. Immediately after I stopped taking Amitriptyline, insomnia was a significant side effect in its own right, but that seems to have faded. It’s the muscle ache/pain, whatever we’re calling it, that’s keeping me awake now. I’m now so sleep-deprived that, honestly, it’s a struggle to function. Although that’s incredibly depressing, it does give me some hope that when the ache eventually settles, I should be able to finally get some sleep.
Where next?
I don’t know. There’s this niggle in the back of my head that I can’t shake off: What if this isn’t withdrawal and this is a reaction to the Fluoxetine? As is generally the case, I started taking Fluoxetine at the same time as reducing Amitriptyline, and all the symptoms I have are common to SSRIs like Fluoxetine, so it’s entirely possible. In that case, nothing will improve, no matter how long I wait. As far as I’m aware, there’s no way of telling.
At the moment, my plan is to wait a few more weeks and see what happens. If things are still the same this time next month, then maybe I need to think again.
Dr Mark Horowitz’s website offers the most practical, professional advice I’ve found online. The academic papers are impenetrable to the non-professional. But he has useful links to newspaper articles which explain things in layman’s terms. The UK mental health charity, Mind, is also a good resource.
It’s important to say, I’m not a Doctor. The following is my personal experience. Please speak to your GP before you make any changes to your medication.
My head hurts! I gave up trying not to look at the clock in the middle of the night weeks ago. I’d read that not knowing the time helps you to get back to sleep. It may work for some people, but it doesn’t make much difference to me. So, I can tell you it’s 3:38 am on Saturday 2 August 2025.
I imagine I can hear my wife sleeping in our bedroom. I still think of it as ‘our’ bedroom, although I’ve been sleeping in the spare bedroom for a while now. It didn’t seem fair to both of us to be awake. We are very fortunate that we have a spare bedroom, or this would be far more unpleasant for both of us.
A Quick Recap
At the end of the last post, I’d been cutting down my Amitriptyline for some time. I was taking 6 mg a day, together with 30 mg Fluoxetine. I was reducing the dose by 1 mg every two weeks. At 2 mg, my eBay scales were not accurate enough to measure a single milligram. So, with some trepidation, I stopped the Amitriptyline completely.
“…spontaneous orgasm may be fun, but not in this context…”
This post has taken me a while to write. So, that was four weeks ago. Without being overdramatic, these few weeks have been awful. I thought the side effects were unpleasant before, but they were nothing compared to going cold turkey.
Before I put you off the prospect of cutting down your medication. It’s important to say that everyone’s experience is different. Some people suffer only very mild side effects. The symptoms tend to be worse the longer you’ve been taking the medication. I had been taking Amitriptyline (it’s quite nice to be able to say ‘had’) for over 25 years.
The UK mental health charity, Mind, has a list of possible side effects of antidepressant withdrawal. With the thankful exception of spontaneous orgasm, which may be fun, but not in this context, I think I’ve experienced all of them.
Where I am now
The worst aspect, for me, is the constant aches and the resultant inability to sleep. At times, it feels as though my whole body has a small electric current running through it. Some nights, I get up multiple times, trying to stretch, quietly wandering the house. I’ve tried taking paracetamol, ibuprofen and Nytol (an over-the-counter sleeping tablet). None of which seems to make much difference.
Sleep deprivation is so pervasive that it overcomes everything else. Under its suffocating blanket of exhaustion, my other side effects may be reducing, but I’m not sure I could tell.
I said last time that I thought Fluoxetine was causing many of my side effects. I’ve since realised that I started taking it at the same time as cutting down my Amitriptyline, so I can’t be sure. Although, my gut feeling is that the Fluoxetine is, at least, partially to blame.
About this time, I had a call from a woman at the local Mental Health Team, asking me if I was happy with the help I’d received. I explained, as politely as possible, that they hadn’t provided any help. We went through the whole thing again. She said she’d call back. Five minutes later, she asked a bunch more questions and told me she’d discuss it with her Supervisor.
The Supervisor called; we started from scratch. When I described the pains in my legs, he said he was concerned about my sodium levels. Apparently, SSRIs can cause reduced sodium levels, which, amongst other things, causes muscle pain. I’ve since had a blood test, and my sodium levels are fine, which, to be honest, I’m slightly disappointed about. It would be great to understand what’s going on. If you’re taking an SSRI and experience muscle pain, it’s worth checking out.
Where next?
I mentioned before, Dr. Mark Horowitz, who wrote the book on antidepressant withdrawal. He says that less than 5% of people continue to experience side effects after nine months. At only four weeks in, that seems like a long wait!
Other than that, I’m not sure. I discussed with the GP cutting down the Fluoxetine and she thinks it’s a good idea, but I’m nervous. At the moment, I don’t need to add to the complications.
Professional Advice
Mark Horowitz’s website offers the most practical, professional advice I’ve found online. The academic papers are impenetrable to the non-professional, but he has useful links to newspaper articles which explain things in layman’s terms. The UK mental health charity, Mind, is also a good resource.
It’s important to say, I’m not a Doctor. The following is my personal experience. Please speak to your GP before you make any changes to your medication.
My head hurts. I’m trying not to look at the clock. It’s still dark; early June in the UK, so maybe 3-4 am? The next thing that comes into my mind are the drugs. In the last six months, I’ve probably spent more time thinking about the drugs than anything else. I’ve become something of an internet expert on the subject.
This tends to be the pattern: for a couple of weeks after reducing my medication, most mornings I wake with a headache, then usually I can’t get back to sleep. I’ve always needed my eight hours, so the cumulative effect of getting only four or five, is beginning to tell. My social life has diminished to almost nothing. Up to this weekend, I’d met one friend this year. There’s an irony, that withdrawing from the drug you take for depression restricts your life to such a degree it’s difficult not to feel depressed.
How I got here
Late last year, I went to see my GP. My long-term IBS and the resulting constipation has been getting worse. The leaflet that comes with medication (the one you usually throw away) is titled ‘Information for the user.’ Information for Amitriptyline ‘users’, is 4,000 words in very small type. In the long list under ‘Possible side effects’ it says, can cause “Bad constipation, a swollen stomach, fever, and vomiting in 1 in 1,000 people”. I’m pleased to say, I wasn’t vomiting, but the connection seemed worth checking out.
“In hindsight, the prospect of a little constipation seemed quite pleasant!”
On Monday morning, I went to see the pharmacist. I explained I’d barely slept for two nights and couldn’t settle. Apparently, the guidance says stopping Amitriptyline, without tapering, should be fine. The pharmacist suggested taking half a dose for a week and try again.
A week later, the headaches were back with a vengeance and I still wasn’t sleeping. I decided to go back on the original dose. My head made it clear it didn’t like me messing about—I had a huge panic attack and the side effects seemed to get worse. In hindsight, the prospect of a little constipation seemed quite pleasant!
Back at the surgery, I saw the GP, not the Registrar. She didn’t like me taking the two drugs together, but wasn’t sure what to recommend. She gave me another prescription for Amitriptyline and referred me to a psychiatric consultant. Which I’m grateful for, it seems to be the only option available, but I’m never going to get to see a psychiatrist. The waiting list is huge and, to be honest, I’d be wasting their time.
This is a textbook case of where recent underfunding of the NHS will cost us all more in the long-run. A recent report by the Royal College of Psychiatrists said that there are 1.6 million people on mental health waiting lists in the UK. They went on to say:
“Mental illnesses can be treated effectively, particularly when they are identified early, but delays to care put people at risk of developing a more complex illness which can harm their long-term health and prevent them from being productive. Worryingly, the number of people waiting for mental-health care has risen by 29% over the last two years, with some waiting for two years or more”.
I am far from an urgent case, and I’m lucky to work from home; there are many mental health implications of long-term home working, but that’s another post. Many days over the past few months I would have been unable to commute to an office. Enough, that, I’m sure, it would have jeopardized my employment. At that point, I stop paying into the system and start needing to take out.
So What Next?
Taking both drugs together was just about tolerable. But I knew I couldn’t continue taking the Amitriptyline long-term, especially mixed with Fluoxetine, which I’d now been taking for a few months. I imagined my neurons, settling in with the new cocktail, one I was going to have to disturb soon.
Dr Mark Horowitz, who wrote the book on antidepressant withdrawal, says, that antidepressants should be reduced by 10% of the previous dose. So, my 25 mg would be 22.5 mg, then 20.5 mg, etc. You can see the problem, drugs aren’t available in infinitely smaller doses. I turn to the web and buy some milligram scales. For a law-abiding middle-aged man, even this online shopping seemed like a risky act. I imagine the Drug Squad kicking my door down at any moment (they didn’t, btw).
I knew the Amitriptyline needed to go, but we’d rubbed along OK; longer than many marriages. It was the Fluoxetine that was spoiling the party. Fluoxetine also comes in handy capsules. Opening those seemed less Breaking Bad, than crushing Amitriptyline tablets with the back of a spoon!
However, out came the spoon and the aluminium foil and over a period of a few weeks, I reduced the Fluoxetine from 40 to 30 mg. But I couldn’t ignore my ever decreasing stash of Amitriptyline; would the GP give me another script? Trust me, it’s a great question to ponder at 4 am.
Facing Reality
The NHS wasn’t going to come charging over the hill to save me any time soon, I needed to bite the bullet. One reality of getting older is the realisation that you have to take responsibility for your own health. You may have a loving partner to help, but it’s your responsibility. So, I’ve slowly been reducing the Amitriptyline. My head is far from happy about it and doesn’t let me forget it. I recently dropped to 6 mg (still with 30 mg of Fluoxetine). I have enough Amitriptyline to give me two weeks between reductions. Not ideal, but at the moment manageable.
I like to think, once I’m completely off of Amitriptyline and my head has had some time to settle, I’ll reduce the Fluoxetine. I’ve been on antidepressants for so long, I don’t know the real extent of my depression. But for the moment going from two drugs to one is the priority. I’ll let you know how that goes!
As I mentioned, Dr. Mark Horowitz offers the most practical, professional advice I’ve found online. The academic papers are impenetrable, to me at least, but he has useful links to newspaper articles. The UK mental health charity, Mind, also has some good advice.